
Three months ago, when we were in the US, we had an appointment with Dr William Mackenzie, an orthopedic surgeon who specialises in skeletal dysplasias. He had a few suggestions as to how to treat Maddy's feet, hips and spine.
In Hong Kong, we see not one orthopedic team, but two. Our spinal team deals with all spinal issues, and the pediatric team deals with everything else. After we returned home, we brought Dr Mackenzie's thoughts to these teams to hear their thoughts.
Our pediatric team was completely on the same page as Dr Mackenzie. For her hips, we will continue to observe them as she grows - her hips are not great, both the head of the femur (thigh bone) and the socket of her hip joint are misshapen but for now, she can use them and any surgery could theoretically worsen that. When she is older, she will need a hip replacement, maybe around age 30 or so. For her feet, our orthopedic doctors agree that the current orthotics don't provide enough support for Maddy's ankles and so this week, she will be fitted for dynamic AFOs.

Dynamic AFOs, pictured above, are basically an "ankle-foot orthotic" with a hinge at the ankle - that way the ankle can bend forwards and backwards, but not sideways. Maddy sometimes has a habit of walking on the inside of her foot, even when she is wearing her orthotics (the TVB Pearl documentary picked up on this and made it look like she always walks like this! She doesn't, only sometimes. But regardless it's not good for her ankles and these will provide better support for them).
Onto the other area of concern: Maddy's spine (see this post for a lovely x-ray of it!). Dr Mackenzie's opinion was that we should start casting Maddy's back to potentially delay the need for surgery. Eventually she would need growing rods to support/correct her scoliosis but the best thing would be to avoid that for as long as possible. The spine has been the major concern for me and was the cause of a nice little meltdown the other day.
When we arrived back in Hong Kong, I saw one doctor on the spinal team. I discussed Maddy's case with him and he recommended against the casting for various reasons. I mentioned Dr Mackenzie's thoughts to him and asked if he could contact him and his response was "I could contact him but it wouldn't make me change my opinion anyway." This response bothered me - but as he was going to refer me to maybe the most senior doctor on the team, I figured I would just let it go and see what the other guy had to say.
I was really excited to meet with this senior doctor - he is very well respected, is a professor and has made some amazing and exciting contributions to spinal surgery. The appointment with him went very well, I thought.
At our first appointment with the spinal team back in January of last year, a doctor there mentioned that Maddy had a hemivertebra. At that stage, it was just a "kink" and the scoliosis had not yet developed. What is a hemivertebra? Have a look at this picture:
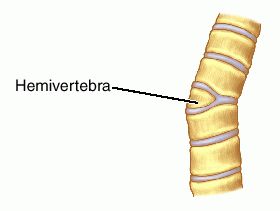 Basically, a hemivertebra is when only half of the vertebra develops. As a result, you see this kind of a "kink" in the spine and the spine then curves into a scoliosis so that the body isn't held at this strange angle.
Basically, a hemivertebra is when only half of the vertebra develops. As a result, you see this kind of a "kink" in the spine and the spine then curves into a scoliosis so that the body isn't held at this strange angle.
Since the hemivertebra had been mentioned before, I didn't question it when this professor brought it up again. Basically, his plan would be within the next 18 months or so, to remove the deformed vertebra and fuse the two vertebra either side of it together. Doing so would remove the source of the scoliosis and theoretically, it would improve the curves in Maddy's spine. He also commented that casting was not likely to be effective in the upper thoracic region where Maddy's main curves are, and that this was our best option at the current time. We planned to do a CT scan to get a better picture of the hemivertebra and to be able to prepare for probable surgery.
I left the appointment feeling quite positive - of course I dread the thought of spinal surgery, but this kind of surgery is far less major than putting rods along her entire spine, and it is a plan - I like to have a plan! I neglected to ask this doctor if he could consult with Dr Mackenzie as I thought I would go home and ask his opinion on this plan myself.
I emailed Dr Mackenzie and waited for his reply. When he wrote back, he told me that he does not believe that Maddy has a hemivertebra, that he would still recommend casting, that he would avoid surgery for now and that he would not recommend having the CT scan as he was quite sure it was not a hemivertebra anyway (it is best to avoid unnecessary CT scans as each scan contains the same level of radiation as something like 100 x-rays). He also confirmed that casting was probably not going to correct the curves in Maddy's upper spine (where her major issues are) but that it was likely to have a positive effect on her less severely curved lower spine.
It is a hard place to be, stuck between two differing opinions of two highly qualified doctors. Not knowing exactly what to do, I emailed our doctor here in Hong Kong with Dr Mackenzie's thoughts and asked if he could please consult with him as to what the best plan would be. I also had probably my biggest melt-down since I was pregnant with Maddy (can I blame pregnancy hormones again?) As a parent, I just want what is best for Maddy and sometimes it is hard to know exactly what that is. Our spinal team here are very good at what they do and they are highly specialised in the spine and in scoliosis. They don't, however, have a great amount of experience in diastrophic dysplasia. Dr Mackenzie on the other hand has maybe more experience than anyone in diastrophic dysplasia - however he deals with the whole body - spine, feet, knees, hips... I figure that if these two experts can communicate together we'd have the best of both.
Ultimately, though, Dr Mackenzie is not our doctor - he is just consulting with our doctors here. And if they (for whatever reason) choose not to avail themselves of his expertise, we cannot force them to communicate with him. I think that our doctor here may try to contact him though - I sincerely hope that he does.
After a few days and a lot of thinking, I've realised though that we still have time to figure this out. As much as I'd like to know the plan right now, the simple fact is this is still up in the air. As for casting, knowing that it will not really help her main curve that much makes it less urgent to me - I am happy for now to leave that alone.
Maddy may or may not have a hemivertebra. The CT scan definitely would help to clear that up so I think if these two experts cannot agree, we would be foolish not to proceed with the CT scan. As to what that shows and what the outcome will be there, we'll figure that out later. "Wait and see" - that seems to be the story of our life!
When we arrived back in Hong Kong, I saw one doctor on the spinal team. I discussed Maddy's case with him and he recommended against the casting for various reasons. I mentioned Dr Mackenzie's thoughts to him and asked if he could contact him and his response was "I could contact him but it wouldn't make me change my opinion anyway." This response bothered me - but as he was going to refer me to maybe the most senior doctor on the team, I figured I would just let it go and see what the other guy had to say.
I was really excited to meet with this senior doctor - he is very well respected, is a professor and has made some amazing and exciting contributions to spinal surgery. The appointment with him went very well, I thought.
At our first appointment with the spinal team back in January of last year, a doctor there mentioned that Maddy had a hemivertebra. At that stage, it was just a "kink" and the scoliosis had not yet developed. What is a hemivertebra? Have a look at this picture:
Since the hemivertebra had been mentioned before, I didn't question it when this professor brought it up again. Basically, his plan would be within the next 18 months or so, to remove the deformed vertebra and fuse the two vertebra either side of it together. Doing so would remove the source of the scoliosis and theoretically, it would improve the curves in Maddy's spine. He also commented that casting was not likely to be effective in the upper thoracic region where Maddy's main curves are, and that this was our best option at the current time. We planned to do a CT scan to get a better picture of the hemivertebra and to be able to prepare for probable surgery.
I left the appointment feeling quite positive - of course I dread the thought of spinal surgery, but this kind of surgery is far less major than putting rods along her entire spine, and it is a plan - I like to have a plan! I neglected to ask this doctor if he could consult with Dr Mackenzie as I thought I would go home and ask his opinion on this plan myself.
I emailed Dr Mackenzie and waited for his reply. When he wrote back, he told me that he does not believe that Maddy has a hemivertebra, that he would still recommend casting, that he would avoid surgery for now and that he would not recommend having the CT scan as he was quite sure it was not a hemivertebra anyway (it is best to avoid unnecessary CT scans as each scan contains the same level of radiation as something like 100 x-rays). He also confirmed that casting was probably not going to correct the curves in Maddy's upper spine (where her major issues are) but that it was likely to have a positive effect on her less severely curved lower spine.
It is a hard place to be, stuck between two differing opinions of two highly qualified doctors. Not knowing exactly what to do, I emailed our doctor here in Hong Kong with Dr Mackenzie's thoughts and asked if he could please consult with him as to what the best plan would be. I also had probably my biggest melt-down since I was pregnant with Maddy (can I blame pregnancy hormones again?) As a parent, I just want what is best for Maddy and sometimes it is hard to know exactly what that is. Our spinal team here are very good at what they do and they are highly specialised in the spine and in scoliosis. They don't, however, have a great amount of experience in diastrophic dysplasia. Dr Mackenzie on the other hand has maybe more experience than anyone in diastrophic dysplasia - however he deals with the whole body - spine, feet, knees, hips... I figure that if these two experts can communicate together we'd have the best of both.
Ultimately, though, Dr Mackenzie is not our doctor - he is just consulting with our doctors here. And if they (for whatever reason) choose not to avail themselves of his expertise, we cannot force them to communicate with him. I think that our doctor here may try to contact him though - I sincerely hope that he does.
After a few days and a lot of thinking, I've realised though that we still have time to figure this out. As much as I'd like to know the plan right now, the simple fact is this is still up in the air. As for casting, knowing that it will not really help her main curve that much makes it less urgent to me - I am happy for now to leave that alone.
Maddy may or may not have a hemivertebra. The CT scan definitely would help to clear that up so I think if these two experts cannot agree, we would be foolish not to proceed with the CT scan. As to what that shows and what the outcome will be there, we'll figure that out later. "Wait and see" - that seems to be the story of our life!
What a tricky situation to be in. it must be very difficult for you when people are recommending two different causes of treatment! We will be praying that your Dr consults the other specialist and that the best possible plan can be made for maddy!
ReplyDelete